
Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality worldwide, underscoring the importance of precise and proactive prevention strategies. Central to effective CVD management is the ability to accurately stratify patient risk and align statin therapy intensity accordingly. This approach requires consideration of both quantitative 10-year ASCVD risk estimates and the presence of key comorbid conditions that independently elevate cardiovascular risk.
This comprehensive overview explores the core principles of CVD risk stratification, the selection of statin intensity based on risk categories and clinical context, and dosing guidelines across common statins. In addition, the article addresses the management of patients who are intolerant to statins, highlighting alternative therapies such as Livalo (pitavastatin) and PCSK9 inhibitors like Repatha (evolocumab). A visual summary is also provided to support clinical decision-making at the point of care.
1. CVD Risk Stratification
1.1 Defining Cardiovascular Disease Risk
CVD risk stratification involves assessing an individual’s likelihood of experiencing cardiovascular events based on various risk factors. These risk factors can be categorized into modifiable and non-modifiable elements. Non-modifiable factors include age, sex, and family history, while modifiable factors take into account lifestyle choices, such as smoking, diet, physical activity, cholesterol levels, and blood pressure.
1.2 Common Risk Assessment Tools
Several tools are available for clinicians to evaluate CVD risk:
- Framingham Risk Score: This model calculates the 10-year risk of developing coronary heart disease based on factors such as age, gender, cholesterol levels, blood pressure, diabetes status, and smoking.
- ASCVD Risk Calculator: Developed by the American College of Cardiology and the American Heart Association, this calculator provides a 10-year risk assessment for atherosclerotic cardiovascular disease events.
- Reynolds Risk Score: This tool factors in additional variables, such as high-sensitivity C-reactive protein levels and family history, making it particularly useful for women and those with a family history of premature cardiovascular disease.
1.3 Implications of Risk Stratification
Understanding an individual’s risk level is integral to developing a tailored prevention and treatment plan. High-risk patients may require more aggressive treatment interventions, including lifestyle changes and pharmacotherapy, while those at lower risk may benefit from less intensive approaches.
2. Statin Intensity and Dosing Guidelines
2.1 Overview of Major Statins
Statins are a class of drugs used primarily to lower cholesterol levels and reduce the risk of cardiovascular events. The following are some major statins commonly prescribed:
- Atorvastatin (Lipitor)
- Rosuvastatin (Crestor)
- Simvastatin (Zocor)
- Pravastatin (Pravachol)
- Lovastatin (Mevacor)
- Pitavastatin (Livalo)
2.2 Statin Intensities
Statins can generally be categorized into three intensities based on their potency and cholesterol-lowering efficacy:
2.2.1 High-Intensity Statins
High-intensity statins are designed to reduce LDL cholesterol by ≥50%. Major high-intensity options include:
- Atorvastatin (40-80 mg)
- Rosuvastatin (20-40 mg)
2.2.2 Moderate-Intensity Statins
Moderate-intensity statins lower LDL cholesterol by 30% to <50% and include:
- Atorvastatin (10-20 mg)
- Rosuvastatin (5-10 mg)
- Simvastatin (20-40 mg)
- Pravastatin (40-80 mg)
2.2.3 Low-Intensity Statins
Low-intensity statins reduce LDL cholesterol by <30%. These include:
- Simvastatin (10 mg)
- Pravastatin (10-20 mg)
- Lovastatin (20 mg)
2.3 Individualizing Statin Therapy
Dosing and intensity of statin therapy should be individualized based on risk stratification. High-risk individuals or those with established CVD typically warrant high-intensity statin therapy, while moderate-intensity may be sufficient for others depending on their specific risk factors.
2.4 Risk Thresholds and Adjustments Based on Comorbidities
The intensity of statin therapy should align not only with calculated CVD risk but also with the presence of specific comorbidities that independently increase cardiovascular risk. Clinical guidelines from the U.S. Preventive Services Task Force (USPSTF) and the American College of Cardiology/American Heart Association (ACC/AHA) provide structured frameworks for determining statin initiation based on 10-year ASCVD risk and clinical context.
2.4.1 Risk-Based Initiation Criteria
- High-Intensity Statins are recommended for:
- Adults with clinical ASCVD (e.g., prior MI, stroke, PAD)
- Adults with LDL ≥190 mg/dL
- Adults aged 40–75 with diabetes and ≥20% 10-year ASCVD risk
- Moderate-Intensity Statins are considered for:
- Adults aged 40–75 with ≥10% 10-year ASCVD risk
- Patients with diabetes and intermediate risk (10–19%)
- Patients aged 40–75 with multiple risk factors even if ASCVD risk is slightly below 10%, after shared decision-making
- Low-Intensity Statins are typically not preferred unless required due to intolerance or in special populations (e.g., very elderly or frail patients)
2.4.2 Key Comorbidities Influencing Statin Intensity
Certain comorbid conditions elevate ASCVD risk and may necessitate more aggressive lipid-lowering therapy, even if traditional risk calculators underestimate their impact:
- Diabetes Mellitus (Type 1 or Type 2)
- Considered a coronary heart disease risk equivalent
- Statin therapy is typically initiated regardless of baseline cholesterol if age 40–75
- High-intensity statins for patients with end-organ damage, long-standing diabetes, or additional risk factors (e.g., hypertension, smoking)
- Hypertension
- Synergistically increases risk of atherosclerosis and stroke
- May elevate patients from borderline to intermediate or high-risk categories
- Chronic Kidney Disease (CKD)
- CKD stage 3 or higher (eGFR <60) is independently associated with higher ASCVD risk
- Moderate- to high-intensity statins recommended for most patients with CKD (non-dialysis)
- Familial Hypercholesterolemia (FH)
- Genetic dyslipidemia leading to extremely elevated LDL-C
- Often requires high-intensity statins + adjunctive therapy such as ezetimibe or PCSK9 inhibitors (e.g., evolocumab)
- Chronic Inflammatory Disorders (e.g., SLE, rheumatoid arthritis, psoriasis)
- Inflammation contributes to accelerated atherosclerosis
- Consider earlier statin initiation even in patients with “normal” LDL levels
- HIV Infection
- Treated as a risk-enhancing factor due to chronic inflammation and medication-related dyslipidemia
- Obstructive Sleep Apnea (OSA)
- Associated with metabolic dysfunction and increased cardiovascular risk
- May tilt the risk-benefit balance toward statin use in borderline-risk individuals
2.4.3 Risk Enhancers in Borderline and Intermediate Risk Groups
The 2018 ACC/AHA guidelines recognize risk enhancers that can guide decisions for patients with a 10-year ASCVD risk of 5–19.9%:
- Family history of premature ASCVD
- Persistently elevated LDL-C (≥160 mg/dL)
- High-sensitivity CRP ≥2 mg/L
- Coronary artery calcium (CAC) score >100 Agatston units
- ABI <0.9
- Ethnicity (e.g., South Asian ancestry)
These factors, in conjunction with patient preference and clinical judgment, support the use of moderate- or high-intensity statins even when calculated risk is not yet ≥10%.
3. Managing Patients Who Cannot Tolerate Statins
3.1 Understanding Statin Intolerance
Statin intolerance is a common barrier to effective lipid management and can manifest as muscle pain, rhabdomyolysis, and other adverse effects. Accurate patient history and assessment are crucial for distinguishing between true intolerance and side effects that may be manageable with alternative strategies.
3.2 Alternative Therapies
For patients who cannot tolerate standard statin therapy, various alternatives can be considered:
3.2.1 Pitavastatin
Pitavastatin is an option for patients with statin intolerance. Its unique pharmacokinetic properties may result in fewer side effects:
- Dosing: Typically prescribed at 1 to 4 mg daily.
- Efficacy: It effectively lowers LDL cholesterol levels and has a favorable safety profile, making it a viable option for those with statin intolerance.
3.2.2 Repatha (Evolocumab)
Repatha, a PCSK9 inhibitor, offers an innovative approach for patients struggling with statins:
- Indications: Recommended for patients with familial hypercholesterolemia or those requiring significant LDL lowering despite maximum tolerated statin doses.
- Dosing: Administered as a subcutaneous injection, commonly in doses of 140 mg every two weeks or 420 mg once monthly.
- Criteria for Use: Generally suitable for patients with a history of cardiovascular events, those with existing coronary artery disease, and those who have not achieved optimal lipid levels on statins.
4. Conclusion
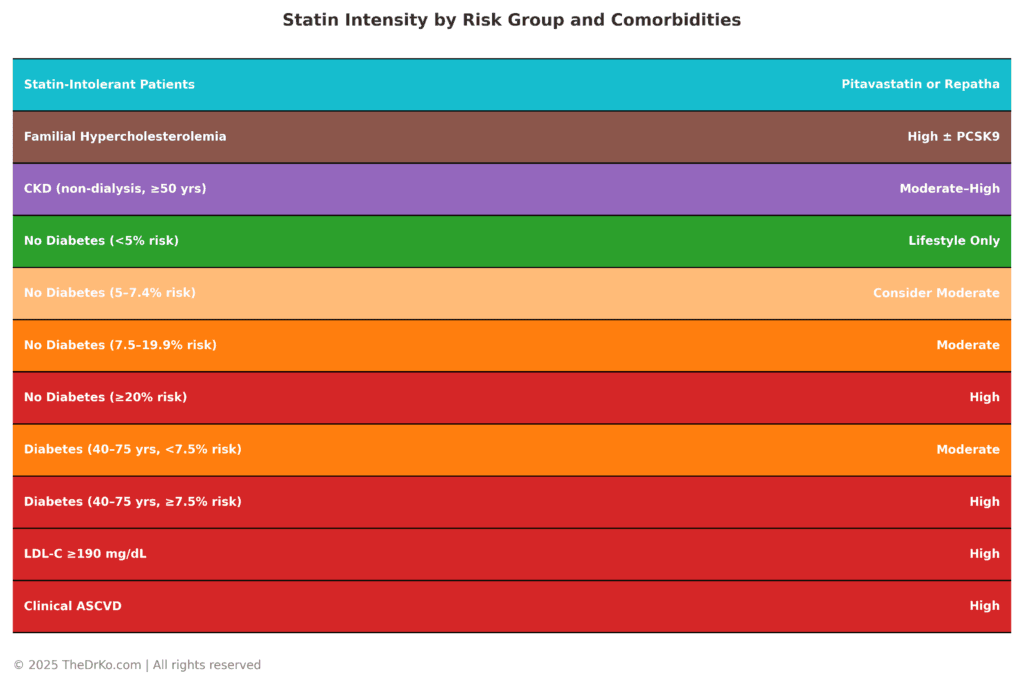
Table: Statin Intensity by Risk Group and Comorbidities
| Patient Group / Risk Category | 10-Year ASCVD Risk (%) | Recommended Statin Intensity | Examples / Notes |
|---|---|---|---|
| Clinical ASCVD (e.g., MI, stroke, PAD) | Not needed (established ASCVD) | High-Intensity | Consider moderate-intensity if ≥75 years or statin intolerance |
| LDL-C ≥190 mg/dL (age 20–75) | Irrelevant | High-Intensity | Consider adding ezetimibe or PCSK9 inhibitor if LDL remains ≥100 mg/dL |
| Diabetes (age 40–75) | ≥7.5% | High-Intensity | Use moderate-intensity if low ASCVD risk and no risk enhancers |
| Diabetes (age 40–75) | <7.5% | Moderate-Intensity | Intensify if other risk factors are present |
| No diabetes, primary prevention (age 40–75) | ≥20% | High-Intensity | Strong recommendation |
| No diabetes, primary prevention (age 40–75) | 7.5–19.9% | Moderate-Intensity | Consider risk enhancers and CAC scoring if decision uncertain |
| No diabetes, primary prevention (age 40–75) | 5–7.4% | Consider Moderate-Intensity | Shared decision-making; look for risk-enhancing factors |
| No diabetes, primary prevention (age 40–75) | <5% | Lifestyle changes only | Statins generally not recommended |
| CKD (non-dialysis, age ≥50) | Irrespective of risk | Moderate- to High-Intensity | Avoid statins if on dialysis unless already taking and tolerating |
| Familial Hypercholesterolemia (HeFH) | Often >20% | High-Intensity ± PCSK9 Inhibitor | Goal: ≥50% LDL reduction; consider combination therapy |
| Statin-Intolerant Patients | Any | Consider Pitavastatin or Repatha | Adjust based on tolerance and LDL goals |
CVD risk stratification, the appropriate choice of statin intensity and dosing, and the management of statin intolerance are foundational elements in comprehensive cardiovascular care. Current guidelines emphasize aligning statin intensity with individual 10-year ASCVD risk, with high-intensity statins reserved for patients with clinical ASCVD, LDL ≥190 mg/dL, or diabetes with high risk.
Comorbid conditions such as diabetes, hypertension, chronic kidney disease, familial hypercholesterolemia, and chronic inflammatory disorders substantially amplify cardiovascular risk and should prompt earlier or more aggressive intervention, even in patients with intermediate calculated risk. Clinicians should incorporate risk-enhancing factors and clinical judgment to guide shared decision-making, especially in borderline-risk populations.
For patients who are intolerant to statins, alternatives like pitavastatin or PCSK9 inhibitors such as Repatha (evolocumab) provide effective LDL-lowering options and can be life-saving in high-risk individuals.
Ultimately, tailoring statin therapy to the patient’s risk profile, comorbidities, and tolerability ensures optimal prevention of cardiovascular events and improves long-term outcomes. Ongoing patient education, follow-up, and monitoring remain critical components of successful cardiovascular risk management.

Be the first to comment